FNA Biopsy
What is an FNA biopsy and why are they important?
An FNA, or fine needle aspiration, biopsy is a common and simple procedure used to sample thyroid nodules. Thyroid nodules are common, especially if someone in your family has a history of thyroid nodules or thyroid disease. Nodules cannot be properly evaluated with physical examination and blood tests alone. The American Thyroid Association recommends FNA biopsy as the procedure of choice for evaluating thyroid nodules and selecting candidates for surgery. Here at our office, the procedure is done under ultrasound guidance to ensure sample accuracy. A very fine needle is used to attain a tissue sample from the nodule in question, and samples are sent to pathology for evaluation. The results are usually back within two weeks.
The pathology results will indicate one of the following findings: benign, non-diagnostic, atypical/suspicious, or malignant. While the vast majority of thyroid nodules are benign (without cancer), a small percentage do contain thyroid cancer. Nationally, there is a 5% chance the pathologist will not be able to give definite benign or malignant diagnosis, and the report will be non-diagnostic. Our office non-diagnostic average is only about 2%. There is also a 1.5-10% national average that the pathologist will read the sample as benign when it is actually malignant, and the report will be a false-negative. Our office false-negative average is only about 1%. While very rare and minimal, there are risks involved with the FNA biopsy procedure including infection, bleeding and hoarseness.
What to expect during the FNA biopsy procedure
If you have nodules, FNA biopsy is the best way to determine what your course of action should be. The American Thyroid Association recommends FNA biopsy as the procedure of choice for evaluating thyroid nodules and selecting candidates for surgery. The procedure is common and simple, and our office performs at least 20 biopsies per week.
At your biopsy appointment, Dr. Azizi will first ultrasound your neck to check for changes in your nodule(s). One of our nurses will give you informed consent of the procedure, and you will sign the paper for the FNA procedure. You will then be taken to the procedure chair that will recline to put your head back and feet up. This will put your neck in an extended position that is best for the procedure. The lights will be turned off so Dr. Azizi can see the ultrasound image clearly. Before the biopsy, your neck will be cleaned with rubbing alcohol and the ultrasound probe placed on your neck to locate the nodule that is being biopsied.
Dr. Azizi will then administer 1cc of Lidocaine 1% with no epinephrine (a local anesthetic) under the skin over that nodule to numb the area. Dr. Azizi will then insert the needle into the nodule in question all while watching the ultrasound screen. This gives assurance that the needle is in fact inside the nodule. He will then aspirate fluid and tissue out of the nodule, and apply it to a sterile slide for the pathologist’s review. The actual procedure will take about 5 seconds. This process is repeated about 3 times to the same nodule to get tissue from different areas of the lesion. We ask that you do not swallow, cough, talk, or breathe deeply while the needle is in your neck. Short shallow breaths through the mouth are best.
After the procedure, your neck will be cleaned and a band-aid placed over the site. You will hold slight pressure to your neck, and in 15 minutes, your blood pressure will be checked. You should not take any blood thinning medicine (like aspirin, Coumadin, plavix, motrin, etc.) the week before or the afternoon of your biopsy. You may ask your doctor for permission to stop your blood thinner. You are free to resume all normal activities the day after the procedure.
Thyroid Nodules
Thyroid nodules are growths on the thyroid gland. They are the most common endocrine problem in the United States, especially in people who have a family history of thyroid disease. Most thyroid nodules do not cause any symptoms, but because 5-7% of thyroid nodules are malignant, it is important to have your thyroid examined.
It gets tricky, because it is difficult to detect nodules by touch or pressure; only about 5% of thyroid nodules can be felt, so many people are unaware they have them. The best diagnostic test is a thyroid ultrasound.
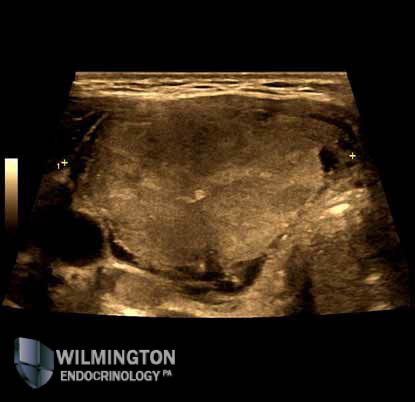
An ultrasound can show what the lesions look like, the size of the lesions, and their location within the thyroid gland. There are specific characteristics about the nodule that can be seen with an ultrasound machine including:
If the lesion is solid, cystic (fluid-filled), or complex (both solid and cystic); hypoechoic, isoechoic, or hyperechoic; and
If the lesion shows calcification, halo sign, or irregular shape or vascularity.
These features help the doctor assess risk for thyroid malignancy. The sonographic features associated with malignant nodules are: hypoechoic thyroid nodules, microcalcifications, irregular shape and margins, and intranodular vascularity.
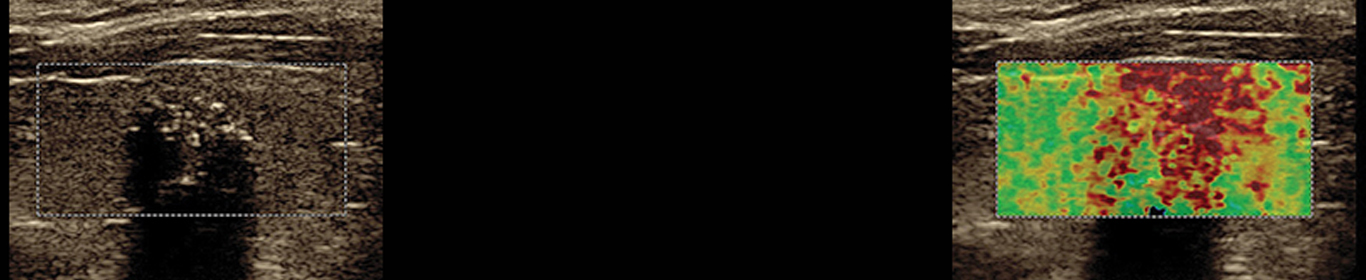
Sonographic features associated with benign nodules are: hyperechoic thyroid nodules, macro or dense calcifications, cystic thyroid nodules, decreased size of nodule over time, and halo sign — a sonolucent rim around the nodule. SonogenicSM nodules are those with high probability for malignancy based on b-mode ultrasound features, strain elastography and shear wave elastography.
Our office utilizes some of the most technologically advanced thyroid ultrasound machines. We emphasize the importance of sonographic features of thyroid lesions in addition to its size to detect malignancy. With the new advanced technology we can examine smaller thyroid nodules, which can lead to early detection of abnormalities.
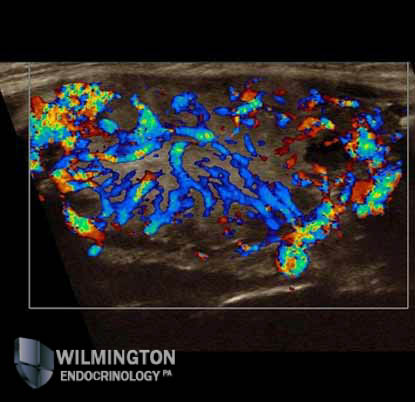
You can see examples of what thyroid nodules look like in the image gallery and video gallery sections of our website. Prior to thyroid nodule biopsy, all nodules will be checked for vascularity, color Doppler, power Doppler, and Elastography. We may perform 3D exam if indicated. We also check for abnormal lymph nodes in the neck.
Ultrasound exams help decide if a nodule should have an FNA biopsy or ultimately surgical excision.
For more information on Thyroid Nodules visit:
The Thyroid Nodules section on the Mayo Clinic website
ATA Patient Education Brochures